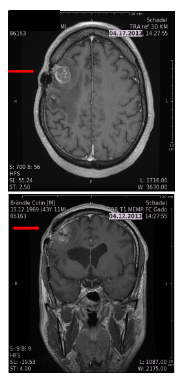
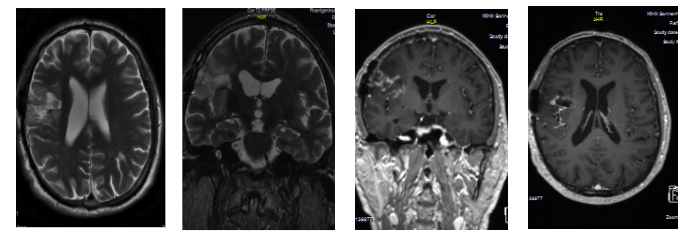
Beginn day 9, resolved day 40 after alpha-therapy: Moderate brachiofacial hemiparesis L, completely resolved, No permanent deficit!
No open surgery
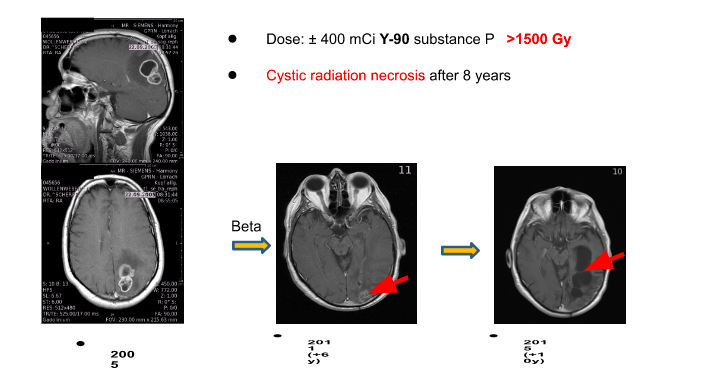
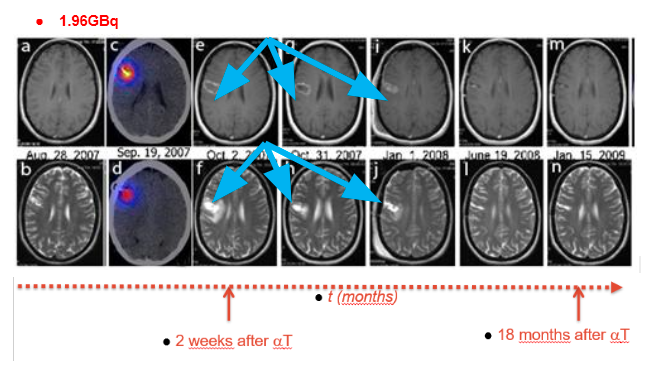
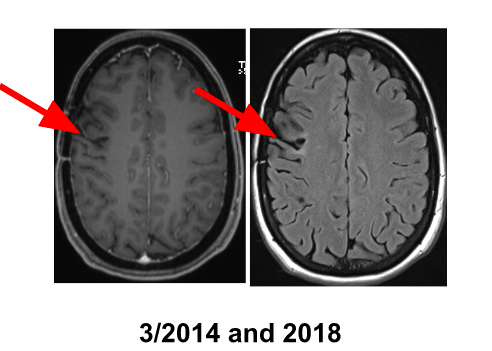
2 years recurrence-free survival in a now 40-year old diffusive infiltrative
astrocytoma grade II patient, no functional deficit, ±“clean“ MRI
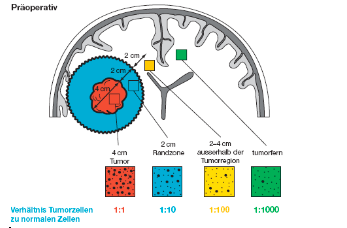
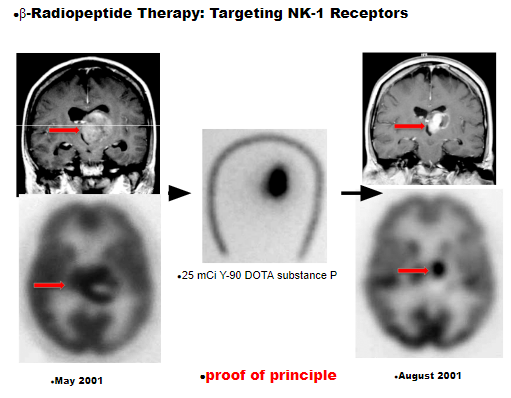
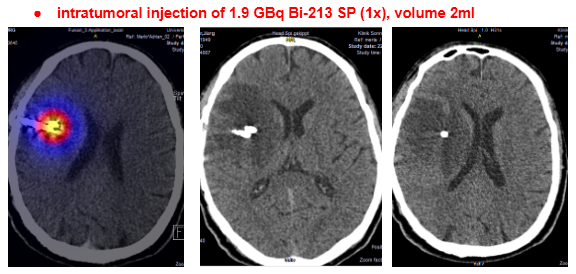
Alpha should not damage neurons, proof of concept: direct injection into motor cortex Can tumor cells infiltrating a functionally critical area of the brain be safely targeted?
Risk of damaging neurons?
Ratio astrocytes to neurons ≈ 10:1
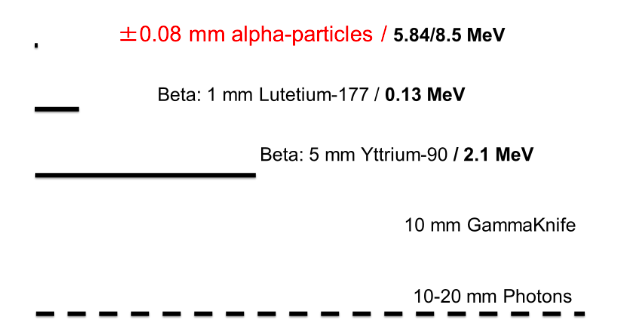
Range: beta 1-5mm alpha: 0.08mm
Alpha particles do not destroy adjacent neurons Minimal damage possible (subclinical) Alpha particles suitable to target functional areas Caveat: repetitive injections, pre-treatment
Alpha should not damage neurons, proof of concept: direct injection into motor cortex Can tumor cells infiltrating a functionally critical area of the brain be safely targeted?
Risk of damaging neurons?
Ratio astrocytes to neurons ≈ 10:1
Range: beta 1-5mm alpha: 0.08mm
Alpha particles do not destroy adjacent neurons Minimal damage possible (subclinical) Alpha particles suitable to target functional areas Caveat: repetitive injections, pre-treatment